B-Scan Interpretation Fundamentals
Master the cross-sectional view. Learn to identify hyper/hypo-reflective signals, layer boundaries, and common scan artifacts.
B-Scan Interpretation Fundamentals
The B-scan is the foundation of all OCT interpretation. Before you can master en face views, you need to read cross-sections fluently. This lesson covers the principles of OCT signal generation and a systematic approach to B-scan analysis.
How OCT Signal Works
OCT measures backscattered light. Structures that scatter light strongly appear bright (hyper-reflective). Structures that transmit or absorb light appear dark (hypo-reflective).
- Hyper-reflective: Nerve fiber layer, EZ, RPE, hard exudates, hemorrhage, fibrosis
- Hypo-reflective: Nuclear layers (cell bodies), cystic spaces, subretinal fluid, photoreceptor outer segments
- Shadowing: Dense structures (hemorrhage, hard deposits) block light and create vertical dark shadows below them
Systematic B-Scan Reading
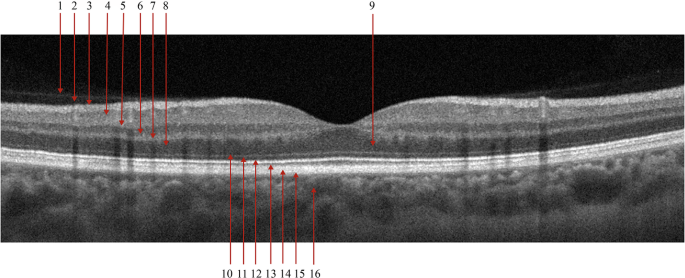
Use this outside-in approach for every B-scan:
- Vitreous: Clear? Cells? Posterior hyaloid visible? Traction?
- Inner retinal surface: ILM smooth? ERM present? Foveal contour normal?
- Inner retina (RNFL → OPL): Normal thickness? Cystic spaces? Hyper-reflective foci?
- Outer retina (ONL → EZ): ELM intact? EZ continuous? Subretinal fluid?
- RPE/Bruch's: Flat? PED? Drusen? Disruption? Atrophy?
- Choroid: Thickness? Vessel dilation? Hyper-reflective lesions?
Fluid Compartments
Fluid location is the single most important diagnostic clue on B-scan:
| Fluid Location | Appearance | Think Of... |
|---|---|---|
| Intraretinal (cystoid) | Round/oval hypo-reflective spaces within retinal layers | DME, RVO, Irvine-Gass, uveitis |
| Subretinal | Hypo-reflective space between EZ and RPE | CSC, wet AMD (CNV), VKH |
| Sub-RPE (PED) | RPE elevation with material underneath | Drusenoid PED (AMD), serous PED (CSC/CNV), hemorrhagic PED |
Hyper-Reflective Foci
Small, bright dots scattered through the retina are hyper-reflective foci (HRF). They represent:
- Migrating RPE cells (in AMD)
- Hard exudate precursors (in DR/DME)
- Inflammatory cells (in uveitis)
- Lipid-laden macrophages
Their location matters: HRF in the outer retina in AMD predict progression to advanced disease.
Scan Quality Assessment
Before interpreting, verify quality:
- Signal strength: Most devices show a quality score. Below threshold, layers blur together
- Motion artifact: Horizontal discontinuities = patient moved during scan
- Segmentation accuracy: Automated layer lines should follow actual boundaries. Errors are common in pathology
- Centering: Is the fovea actually centered? Off-center scans miss pathology
Key Takeaways
- OCT measures backscattered light — bright = high scatter, dark = low scatter
- Use a systematic outside-in approach for every B-scan
- Fluid compartment (intraretinal, subretinal, sub-RPE) is the most important diagnostic clue
- Always check scan quality before interpreting
- Everything you see on B-scan generates contrast on en face — this is the bridge to the next lesson
Educational illustration — B-scan fluid compartments: normal (left), intraretinal fluid DME (center), subretinal fluid CSC (right). Not a clinical scan.
Sign up to track your progress and access all lessons.
Create Free Account