Retinal Layer Anatomy & Normal Findings
Understand the 10 retinal layers visible on OCT and what normal architecture looks like before learning pathology.
Retinal Layer Anatomy & Normal Findings
Before you can identify pathology on OCT, you need to know what normal looks like. This lesson walks through the 10 retinal layers visible on spectral-domain OCT and establishes the baseline architecture you'll reference for every scan you read.
The 10 Layers (Internal to External)
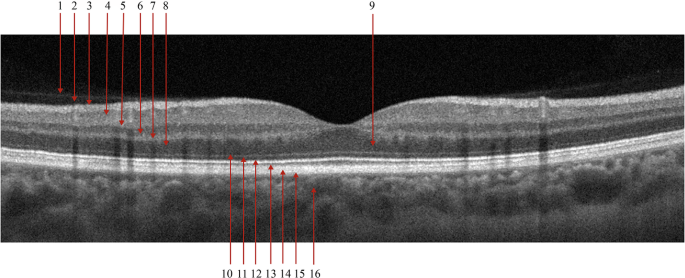
On a standard SD-OCT B-scan, the retina presents as alternating hyper-reflective (bright) and hypo-reflective (dark) bands. Each band corresponds to a specific anatomical structure:
| # | Layer | Reflectivity | Clinical Significance |
|---|---|---|---|
| 1 | ILM (Internal Limiting Membrane) | Hyper-reflective | Boundary for ERM, vitreomacular traction |
| 2 | RNFL (Retinal Nerve Fiber Layer) | Hyper-reflective | Glaucoma assessment, RNFL thickness mapping |
| 3 | GCL + IPL (Ganglion Cell + Inner Plexiform) | Hypo-reflective | Ganglion cell complex, early glaucoma marker |
| 4 | INL (Inner Nuclear Layer) | Hypo-reflective | Bipolar/Muller cell bodies, microcystic changes |
| 5 | OPL (Outer Plexiform Layer) | Hyper-reflective | Henle fiber layer at fovea, hard exudate location |
| 6 | ONL (Outer Nuclear Layer) | Hypo-reflective | Photoreceptor nuclei, thickened in CSC |
| 7 | ELM (External Limiting Membrane) | Hyper-reflective | Photoreceptor integrity marker |
| 8 | EZ (Ellipsoid Zone / IS/OS) | Hyper-reflective | KEY indicator of photoreceptor health |
| 9 | IZ (Interdigitation Zone) | Hyper-reflective | Photoreceptor outer segment tips |
| 10 | RPE/BM (RPE + Bruch's Membrane) | Hyper-reflective | Drusen, PED, geographic atrophy |
The Foveal Contour
At the fovea, the inner retinal layers (RNFL through INL) are absent — they're displaced laterally to create the foveal pit. This is normal. What remains at the foveal center is the outer retina: ONL, ELM, EZ, IZ, and RPE.
Key measurements at the fovea:
- Central foveal thickness (CFT): ~250 μm (varies by device and ethnicity)
- Foveal pit depth: The pit should be symmetric and well-defined
- EZ band: Should be continuous and unbroken across the fovea
The Choroid
Below the RPE, the choroid appears as a heterogeneous band with varying reflectivity. Enhanced depth imaging (EDI-OCT) or swept-source OCT improves choroidal visualization. Normal subfoveal choroidal thickness is approximately 250-350 μm but decreases with age.
In en face imaging, the choroid becomes critically important — it's where you'll see:
- Pachychoroid spectrum disorders (thick choroid with dilated vessels)
- Haller's layer vessels (large choroidal vessels)
- Choriocapillaris flow patterns on OCTA
Vitreous Interface
Above the ILM, you may see the posterior vitreous face. In a complete posterior vitreous detachment (PVD), it appears as a hyper-reflective line separated from the retinal surface. Incomplete PVD with residual adhesion at the fovea is a setup for vitreomacular traction (VMT).
What to Look For on Every Scan
Before analyzing pathology, run through this mental checklist on every OCT:
- Scan quality: Signal strength adequate? Any motion artifact?
- Foveal contour: Symmetric pit? Flattened? Elevated?
- Layer integrity: Is the EZ band continuous? Any disruptions in ELM?
- Fluid: Intraretinal (cystic spaces)? Subretinal (between EZ and RPE)? Sub-RPE?
- RPE: Smooth? Elevated (PED)? Disrupted? Attenuated?
- Vitreous interface: Attached? Detached? Traction?
Key Takeaways
- The retina has 10 distinct layers on OCT, alternating in reflectivity
- The EZ band (ellipsoid zone) is your single most important layer for assessing photoreceptor health
- The foveal pit is normal — inner layers are absent at the center
- Always check: quality, contour, layers, fluid, RPE, vitreous
- Normal measurements vary by device — use normative databases, not memorized numbers
Educational illustration — Retinal layer anatomy: 10 layers from ILM to choroid (left: normal; right: common pathology sites). Not a clinical scan.
Sign up to track your progress and access all lessons.
Create Free Account