RVO & CSC: Basic OCT Patterns
Retinal vein occlusion and central serous chorioretinopathy. Fluid patterns, choroidal changes, and monitoring strategies.
RVO & CSC: Basic OCT Patterns
Retinal vein occlusion and central serous chorioretinopathy both cause macular fluid, but the pathophysiology, fluid compartment, and treatment approach are entirely different. OCT — especially en face — distinguishes them clearly and drives management.
Retinal Vein Occlusion (RVO): OCT Findings
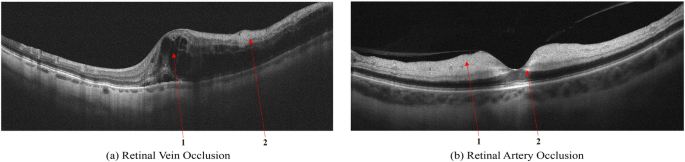
RVO causes venous outflow obstruction — blood backs up, retinal capillaries become hyperpermeable, and fluid accumulates within the retinal layers. The two major types have distinct OCT presentations:
| Feature | BRVO (Branch) | CRVO (Central) |
|---|---|---|
| Fluid distribution | Sectoral — one or two quadrants | Pan-macular, symmetric |
| Cyst morphology | Smaller cysts, often paracentral | Large cysts, often involving fovea |
| Retinal thickening | Asymmetric — follows vein territory | Diffuse, often severe (>500 μm) |
| Outer retinal changes | EZ relatively preserved early | EZ frequently disrupted |
| HRF / Hard exudates | Common at area of stasis | Common throughout posterior pole |
On en face imaging, BRVO produces a sectoral pattern of dark cysts that maps beautifully to the affected vein territory — the geographic boundary is typically sharp at the affected vein's drainage zone. CRVO shows diffuse, bilateral intraretinal cysts across the macula.
Central Serous Chorioretinopathy (CSC): OCT Findings
CSC is fundamentally a choroidal disease — pachychoroid and abnormal choroidal permeability lead to RPE breakdown and subretinal fluid accumulation. The key OCT features:
- Subretinal fluid (SRF): The hallmark. A smooth, dome-shaped clear space between the outer surface of the photoreceptors (EZ) and the RPE. The fluid itself is optically empty (hypo-reflective).
- RPE detachment (PED): Often present — flat, serous PED adjacent to the SRF. In CSC, the PED is typically serous (clear fluid beneath RPE) rather than drusenoid.
- Pachychoroid: Thickened choroid (>300–350 μm subfoveal), dilated Haller layer vessels. Best seen on EDI-OCT or SS-OCT.
- RPE atrophy / pigment changes: In chronic CSC (>3–4 months), secondary RPE changes develop — irregular RPE signal, hyperreflective foci, RPE atrophy on en face
- No intraretinal fluid (in acute CSC): The retinal layers above the SRF are typically normal. The absence of IRF helps distinguish CSC from wet AMD.
CSC vs. Wet AMD: The Critical Differential
Subretinal fluid in a middle-aged patient raises two differential diagnoses: CSC or occult CNV (type 1 MNV). The distinction has major treatment implications:
| Feature | CSC | Type 1 CNV (occult wet AMD) |
|---|---|---|
| Patient age | 30–55 years, male-predominant | Typically >55, equal sex |
| SRF characteristics | Smooth dome, clear | May be more irregular |
| RPE elevation | Serous PED, smooth | Fibrovascular PED, irregular |
| Choroidal thickness | Increased (pachychoroid) | Variable, often thinner in late AMD |
| Drusen | Absent (no AMD) | May be present |
| Hyperreflective material sub-RPE | Absent | Fibrovascular tissue present |
Monitoring Protocols
- Acute RVO: Monthly OCT with anti-VEGF (per SCORE2/BRAVO/CRUISE protocols); assess for non-perfusion concurrently
- Chronic RVO (stable): Every 2–3 months after stabilization; earlier if symptoms change
- Acute CSC: OCT at 6–8 weeks — majority resolve spontaneously. If persists >3 months, refer for photodynamic therapy (PDT) evaluation
- Chronic CSC: Every 3 months; monitor for secondary CNV (occurs in ~5–10% of chronic cases)
Key Takeaways
- RVO = intraretinal fluid (cystoid) in the territory of the affected vein
- CSC = subretinal fluid (smooth dome) + pachychoroid, no intraretinal cysts
- EZ disruption in RVO predicts poor visual recovery — treat promptly
- CSC vs. wet AMD differential is critical — pachychoroid and age help distinguish
- Chronic CSC (>3 months) warrants PDT evaluation and monitoring for secondary CNV
Educational illustration — RVO cystoid IRF (blue) vs. CSC subretinal fluid dome (cyan) and RPE detachment (indigo). Real clinical scans in full course.
Sign up to track your progress and access all lessons.
Create Free Account